Basic QC Practices
2021 QC Survey Results for Hematology
The 2021 Global QC Survey reveals major differences between the hematology and chemistry sections in laboratories around the world.
The 2021 Hematology Global QC Survey Results
Sten Westgard, MS
December 2021
[This survey was completed with the support and partnership of Technopath Clinical Diagnostics.]
- The Top Ten Findings of the 2021 Global QC Survey
- The 2021 Global QC Survey
- The 2021 US QC Survey Results
- The 2021 Asia QC Survey Results
- The 2021 Middle-East QC Survey Results
- The 2021 Latin and South America QC Survey Results
- The 2021 European QC Survey Results
Do Hematology sections use the same old QC rules?
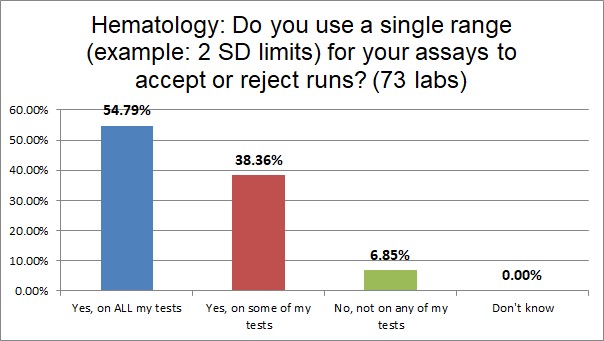
A majority of hematology sections use single ranges like 2 SD on all their tests, but this is 10% less than what's found in chemistry sections. However, only half as many hematology labs do NOT use those ranges on any of their tests.
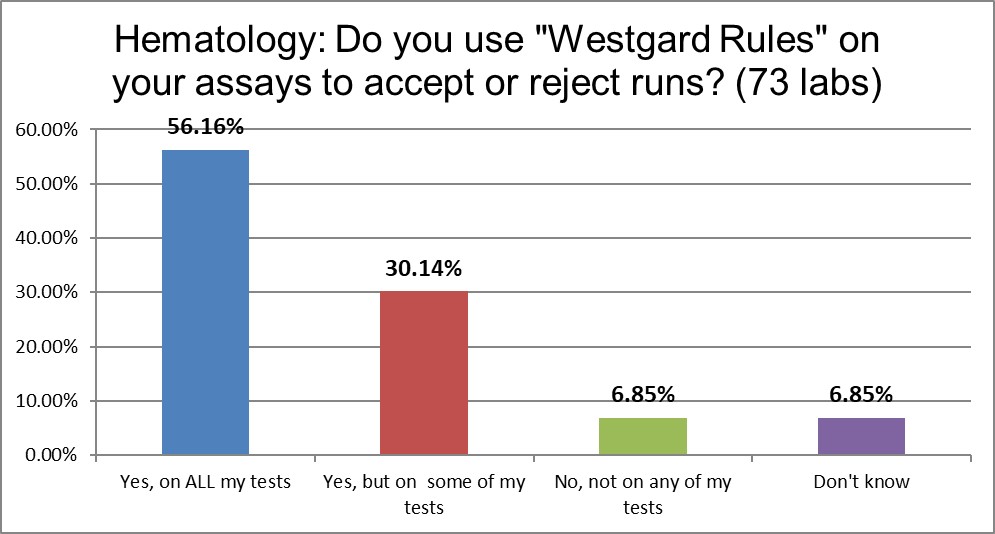
Close to 90% of the hematology sections use "Westgard Rules" on some or all of their tests. But there is more than a 10% difference on who uses a multirule approach on all of their tests. Hematology use of Westgard Rules is lower in this respect by more than 10%.

Almost 50% of hematology sections establish their own mean and SD, almost 20% less than chemistry sections. Close to 60% of hematology sections use manufacturer ranges, which is slightly higher than the chemistry sections. And over 10% of hematology labs are using measurement uncertainty to set their ranges.
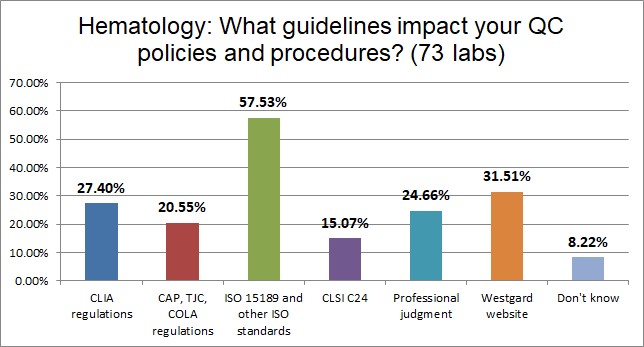
ISO 15189 maintains its global dominance as the most influential standard for setting up hematology control charts. In fact, it has 10% more impact on hematology sections than it does on chemistry sections.

Not surprisingly, the use of manufacturer controls absolutely dominates hematology, 15% higher than what we see for the chemistry sections. Third party assayed liquid controls are a distant second. This is a real divergence of practice. In chemistry, the emphasis on getting independent controls is much stronger.
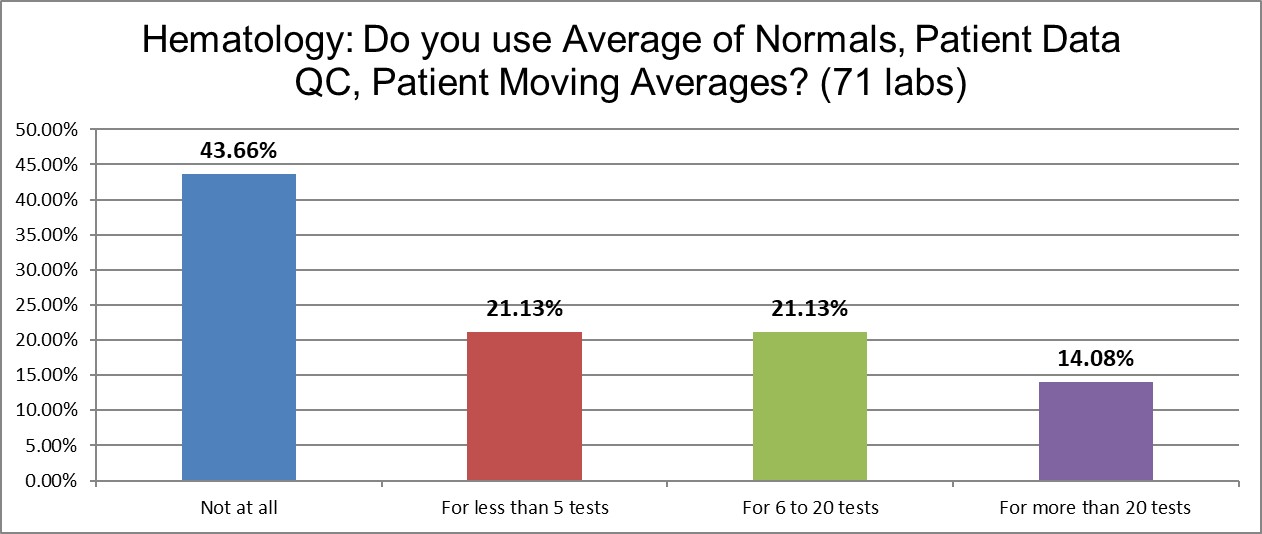
Hematology, which is famous for its use of Bull's algorithm, has the highest use of patient data techniques (commonly called PBRTQC these days). Still, to see over 40% of sections not using those techniques is interesting.
The Real Practice of Running Controls
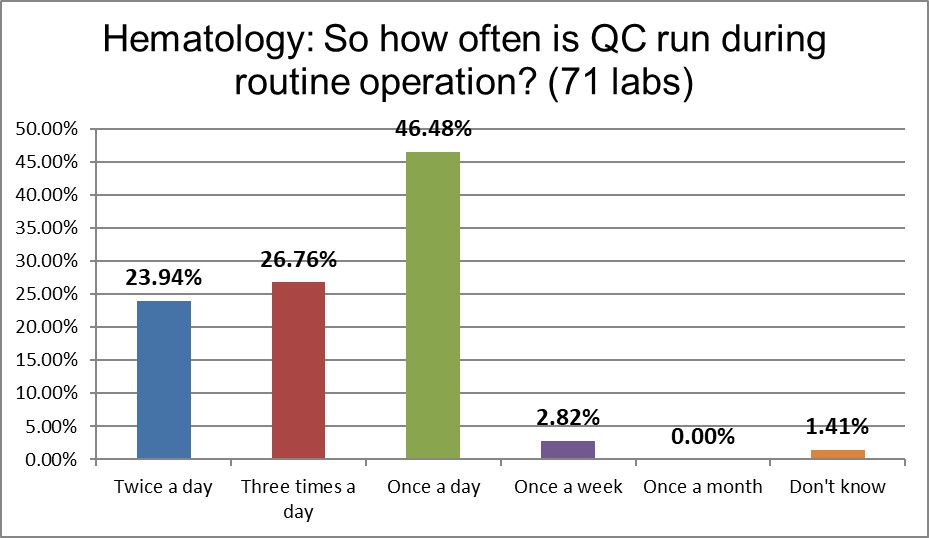
Once-a-day QC is the practice of a majority of chemistry sections, but a minority of hematology labs. Of course, regulations often mandate this more common frequency. The biggest difference between hematology and chemistry is that the former are 10% more likely to be running controls three times a day.
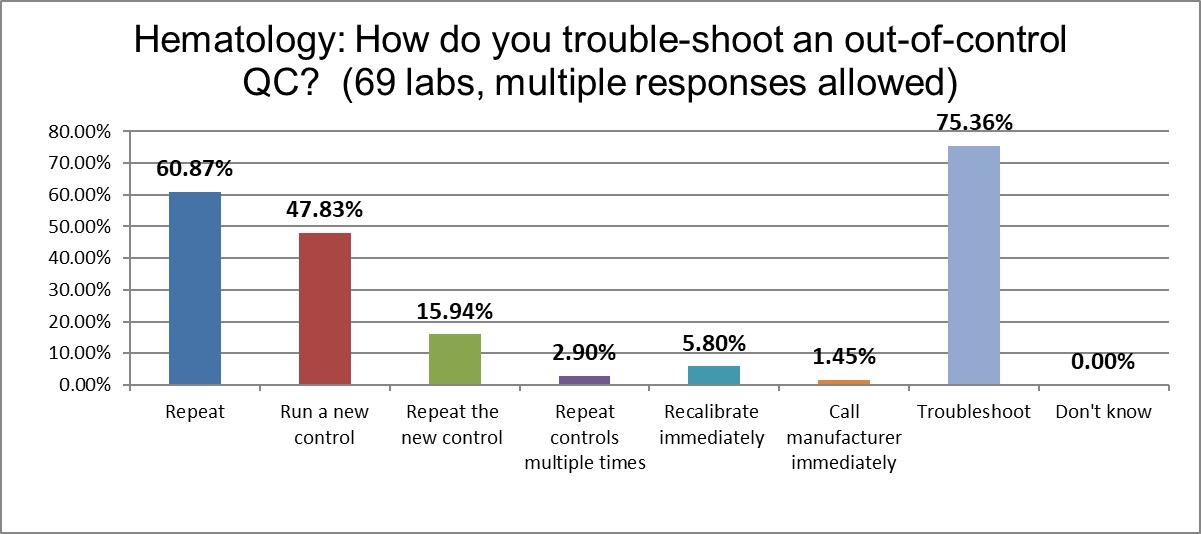
Similar to chemistry, 3 out of 4 hematology sections try to troubleshoot first, repeat second. The bad practices of repeating controls and running new controls are significantly less practiced in hematology, however. Is this because errors happen less in hematology, so are taken more seriously? Or do errors just happen so often in chemistry that they are treated with less concern? That's an area our survey cannot determine.
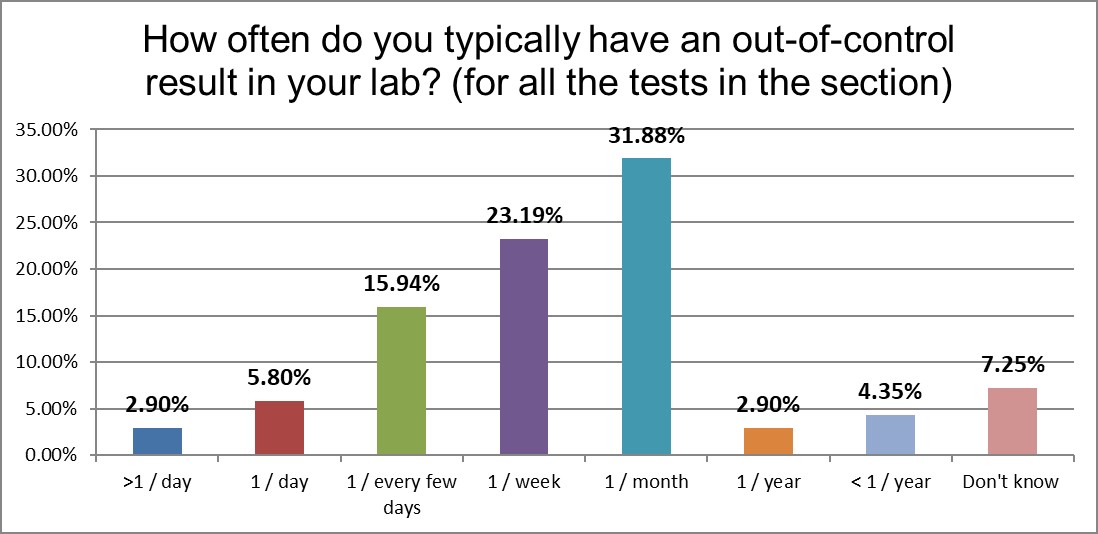
Here we start to see some of the answer. Hematology sections report encountering significantly fewer errors than chemistry sections. Chemistry sections report seeing daily errors 4x more often than hematology. Chemistry sections report seeing errors every few days twice as often as hematology sections. Are hematology instruments that much better than chemistry instruments? Or is there a fundamental difference in practices?
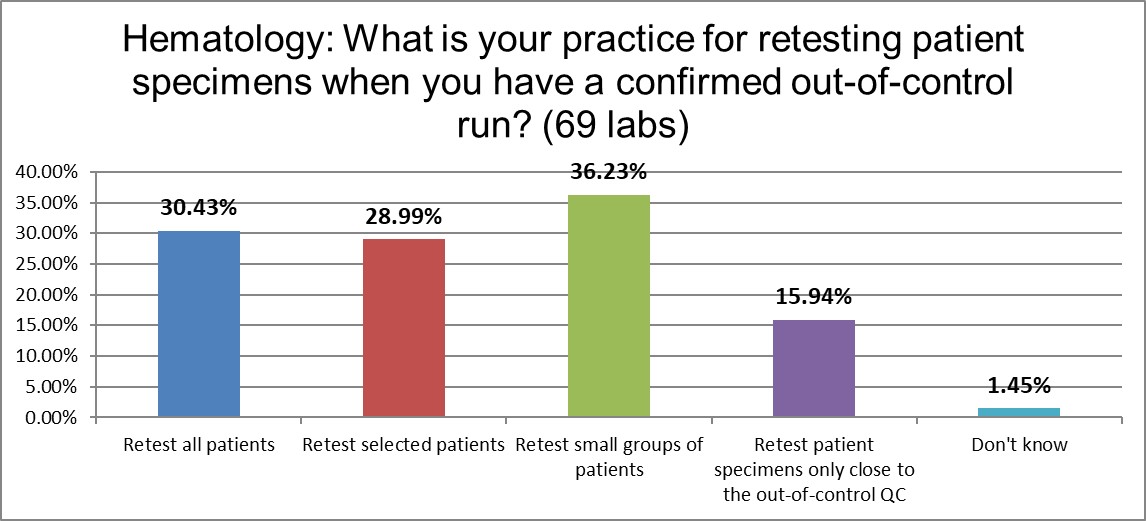
When it comes to retesting patients, hematology practices are equally spread across the major options, retesting all, retesting selected patients (like abnormals), and retesting small groups of patients sequentially. Here is another area of similarity between chemistry and hematology. Once they have a confirmed error, they treat patients similarly.
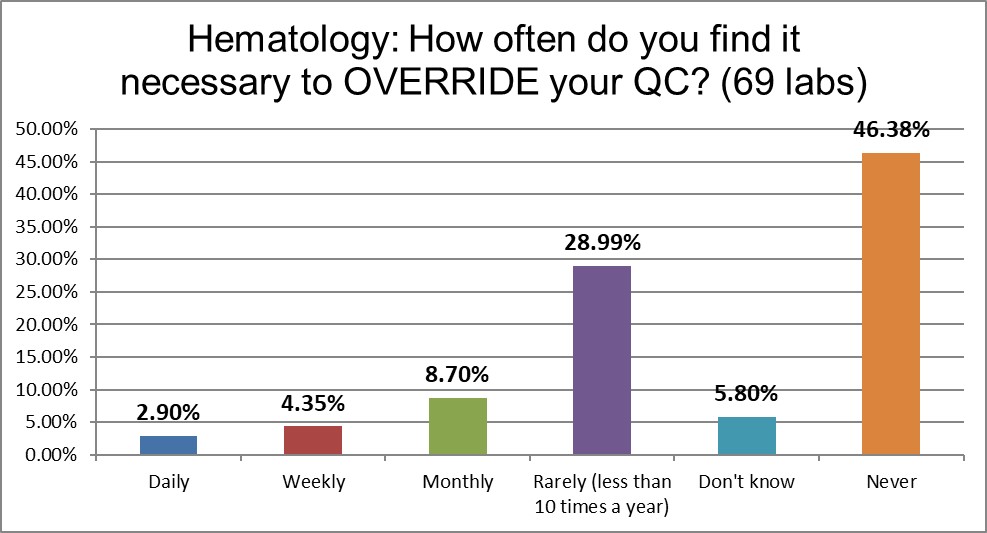
While almost 1 in 8 chemistry sections has to regularly (daily or weekly) override their QC results, this happens only to almost 1 in 14 hematology sections. Chemistry sections are 60% more likely to override their QC than hematology sections. Is that because the instruments are so different in performance? Or that their habits are so different?
The Final Overview
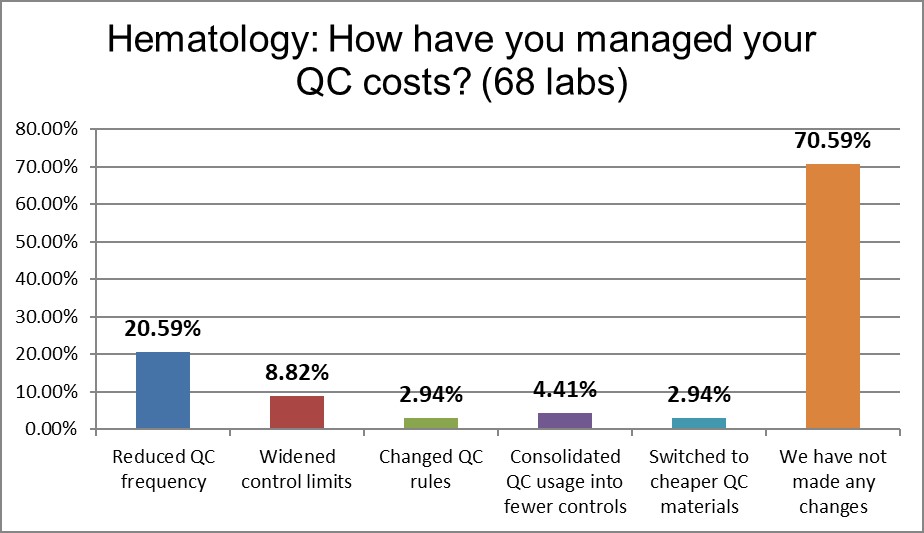
Hematology sections a significantly more likely to have done nothing to change their QC practices. Recalling the dominance of manufacturer controls, it's not surprising to also see that there much fewer changes in controls (consolidation and cheaper controls). The most popular action, for those sections that took action, was to reduce QC frequency. Hematology sections are 25% more likely to have reduced their QC frequency.